



On Monday, America First Legal (AFL) launched a new investigation into the Biden-Harris White House and the National Institutes of Health (NIH) regarding their reckless promotion of youth “gender-affirming” care—a euphemism for experimental chemical castration and genital mutilation—while simultaneously funding studies on the potential long-term harm that it causes to children and adolescents.
AFL’s new investigation follows the work of Children’s Health Defense (CHD) relating to research grants from the NIH, which reveals that giving children and adolescents puberty blockers, sex hormones, and surgical operations may potentially cause irreversible, life-changing harm to children and adolescents.
Based on the records obtained by CHD, the Biden-Harris NIH was clearly aware that:
- There was only “scant data” available on the long-term physiological impact of taking puberty blockers during early puberty, while preliminary studies already reported lower bone mineral density for children taking puberty blockers;
- There is also very limited data on the long-term psychosocial outcomes of “transgender youth” initiating any “gender-affirming” medical care;
- There is “a significant gap” in the current evidence regarding best practices for the healthcare needs of “transgender adults” after surgery—and even less for children and adolescents;
- NIH-funded researchers predicted that their study would show that boys taking estrogen for “gender-affirming” care earlier would become increasingly predisposed to blood clots the longer they took estrogen.
Based on these disturbing revelations, AFL is investigating the extent to which the Biden-Harris White House was as informed as the NIH of these risks while recklessly promoting youth “gender-affirming” care. Specifically, AFL is now seeking communications between the relevant political leadership at NIH and the White House regarding the potential harm to children and adolescents that may be caused by:
- “gender-affirming” hormone (GAH) therapy, i.e., sex hormone therapy with testosterone or estrogen;
- “pubertal suppression” with “gonadotropin-releasing hormone analogists” (GnRHa), i.e., “puberty blockers;” or
- “gender-affirming” surgery or sex reassignment surgery (SRS).
Background: CHD’s investigation reveals that the scientific community poorly understood the long-term effects of youth “gender-affirming” care and anticipated their studies would show medical harm.
CHD, through open records requests, obtained grant application materials that led to the following NIH grants to perform the following studies:
- A $9.7 million award from NIH to Children’s Hospital of Los Angeles (CHLA) to study the impact of early medical treatment in transgender youth;
- A $2.8 million award from NIH to Visiting Nurse Service of New York (VNSNY) to study the long-term healthcare needs of “gender minority” individuals after surgery, their psychosocial adjustment during this phase of their identity development, their quality of life, and long-term physical and emotional wellbeing;
- A $1.7 million award from NIH to Cincinnati Children’s Hospital Medical Center (CCHMC) to study thrombosis risk in transgender adolescents and young adults starting “gender-affirming” hormone therapy.
AFL’s investigations cite the following shocking statements in these grant application materials obtained by CHD:
Statements by the Children’s Hospital of Los Angeles (CHLA):
CHLA’s grant application highlights the “scant evidence-base currently guiding the clinical care of” transgender youth.”
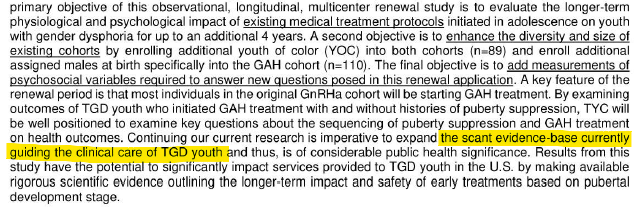
Existing studies had focused on the impact of “gender-affirming” care on adults, but until this study, “no known US studies have examined similar outcomes among transgender youth with gender dysphoria.”
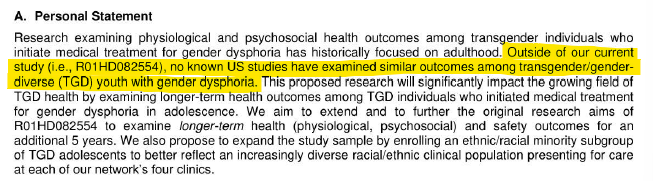
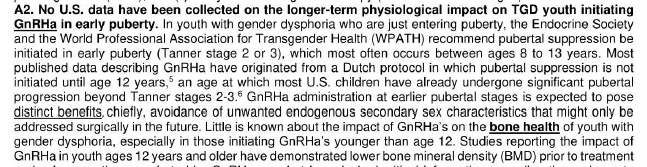
At the time of the CHLA grant application, no U.S. data had been collected on the longer-term physiological impact on transgender youth initiating puberty blockers during early puberty. In comparison, some studies had already reported lower bone mineral density for children taking puberty blockers.
Similarly, no data extending beyond 24 months had been published in the United States on the longer-term physiological effects on transgender adolescents taking sex hormones, particularly under the age of 16, while previous studies had shown a higher incidence of cardiovascular events in adults taking sex hormones.
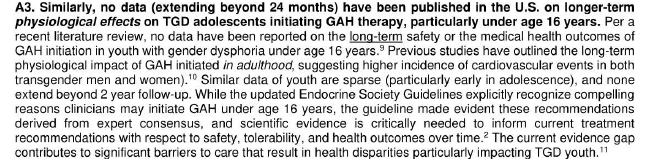
Like the lack of data on the physiological effects, very limited data also exist on the longer-term psychosocial outcomes of transgender youth initiating any “gender-affirming” medical care.

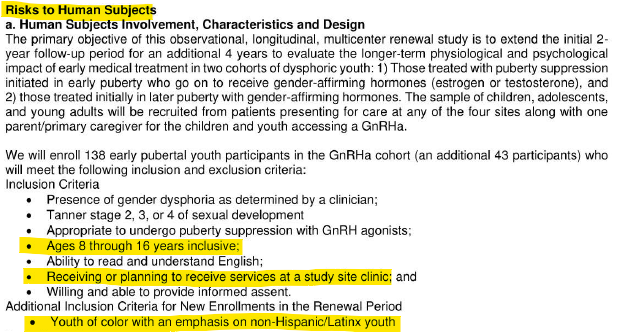
To collect data, this NIH-funded study set out to “enroll 138 early pubertal youth participants” in the puberty-blocker cohort, ages 8 through 16, who are either receiving “or planning to” receive “gender-affirming” care. “Youth of color with an emphasis on non-Hispanic/Latinx youth” (e.g., Black or Asian) was an additional inclusion criterion for enrollment.
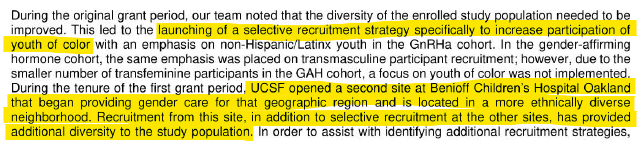
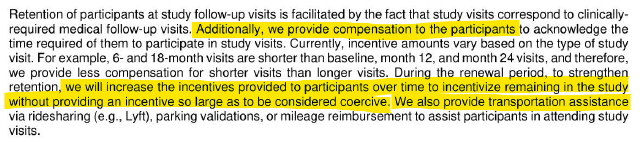
Not satisfied with the racial diversity of the study population, the researchers “launch[ed] a selective recruitment strategy specifically to increase participation of youth of color” by opening another site in Oakland, California. This patronizing attitude regarding race and color mirrors the CDC’s recommendation to use “Black Twitter” to promote COVID-19 vaccination by “disseminat[ing] messages and conduct[ing] outreach in a trusted and culturally responsive and linguistically appropriate way.” The CHLA researchers also provided transportation assistance and increased monetary incentives over time.
Although the scientific community lacked the evidence to assure that youth “gender-affirming” care does not cause long-term medical harm, the radical trans movement continued to push forward with its agenda of transitioning children and adolescents.
Statements by the Visiting Nurse Service of New York (VNSNY):
The VNSNY grant application similarly highlighted the “dearth of evidence on the healthcare needs of [transgender] individuals after surgery” and the “significant gap in the current evidence on best practices.”
Even so, this study did not attempt to examine the life-changing consequences of “gender-affirming” surgeries on minors.
Statements by the Cincinnati Children’s Hospital Medical Center (CCHMC):
The CCHMC grant application highlighted the “unknown” risk of thrombosis (blood clots) for transgender youth taking estrogen due to the lack of long-term studies.
CCHMC goes on, “given the lack of clear data about the thrombotic risk and the absence of clinical guidelines, clinicians are likely to exhibit variability in practice that may adversely impact patient outcomes.”
Furthermore, existing studies on the thrombotic risk for transgenders taking estrogen did not include transgendered youth, who will end up taking estrogen “for a much longer time than TG adults.”

While it seems obvious that a boy who begins taking estrogen earlier in his life would eventually end up with a higher risk of thrombosis, the CCHMC researchers point out that no studies had actually evaluated this connection.

Even the CCHMC researchers hypothesized that their study would show that the youth receiving estrogen for “gender-affirming” care would become increasingly predisposed to blood clots the longer they take estrogen.

Seemingly, without regard for ethics, the NIH-funded study proceeded anyway, with the anticipated result that the test subjects would see an increased risk of blood clots.
AFL recently revealed that the Food and Drug Administration (FDA) Division of General Endocrinology recommended the FDA approve puberty blockers for children despite direct knowledge that these drugs increase the risk of depression and suicidality. Ignoring “the science” and the serious potential risks involved with “gender-affirming” care for children and adolescents, the Biden-Harris Administration fought to challenge state legislation restricting youth access to “gender-affirming” care and instead promoted this dangerous ideology for “how it improves the mental health and overall well-being of gender diverse youth.”
To shed light on the extent to which the Biden-Harris White House was informed of the potential risks by NIH, AFL has requested all communications between the relevant political leadership at NIH with the White House regarding the potential harm to children and adolescents that may be caused by “gender-affirming” care.
Statement from Gene Hamilton, America First Legal Executive Director:
“We are committed to exposing the intellectual and moral rot that is subjecting children to experimental procedures and medical treatments based on the mere belief–contrary to all of human history–that a human being can change their sex without any consequences. The profit-driven sickness that is at the heart of so much of today’s medical community apparently knows no moral boundaries, with many being more than happy to exploit the fantasies of confused people, including minors, so as to be able to make a few more dollars. The American people deserve to know the truth, and we will provide them with all of the information that we can possibly obtain,” said Gene Hamilton.
Statement from Mary Holland, CEO of Children’s Health Defense:
“Children’s Health Defense is happy to provide this FOIA information to AFL for further analysis and investigation. The public needs to understand fully the government’s policies on transgenderism, especially as it relates to children. We need to understand what the government knows, plans, and may be keeping from the public,” said Mary Holland.
Read the document productions here, here, and here and the FOIA here.












{kind=link}